Thoracic inlet
The superior thoracic aperture refers to the opening at the top of the thoracic cavity. It is also referred to anatomically as the thoracic inlet
Borders
- first thoracic vertebra (T1) posteriorly,
- the first pair of ribs laterally
- the superior border of the manubrium anteriorly.
Contents
- trachea
- esophagus
- thoracic duct
- apexes of the lungs
- nerves
- phrenic nerve
- vagus nerve
- Recurrent laryngeal nerves
- sympathetic trunks
- arteries
- left and right common carotid arteries
- left and right subclavian arteries
- veins
- internal jugular veins
- brachiocephalic veins
- subclavian veins
- lymph nodes and lymphatic vessels
Mediastinum
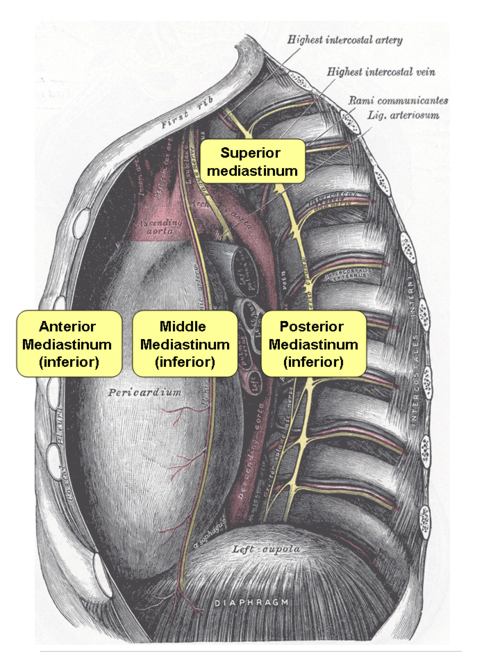
Annotated version of Gray’s image 969; opened Mediastinum viewn from right lateral
The mediastinum lies between the right and left pleurae in and near the median sagittal plane of the chest. It extends from the sternum in front to the vertebral column behind, and contains all the thoracic organs except the lungs. It may be divided for purposes of description into two parts: an upper or superior part and a lower or inferior part.
- Superior Mediastinum
The superior mediastinum extends from the upper level of the pericardium with its upper limit at the superior thoracic aperture and its lower limit at the thoracic plane which runs from the sternal angle (the joint between the manubrium and the body of the sternum) to the intervertebral disc of T4-T5. The (transverse) thoracic plane divides the mediastinum into these upper and lower parts.
- Inferior Mediastinum
The inferior mediastinum extends below the upper level of the pericardium onto the diaphragm. This lower part is subdivided into three regions all relative to the pericardium. The anterior mediastinum is in front of the pericardium. The middle mediastinum contains the pericardium and its contents. The posterior mediastinum is behind the pericardium.
Anatomy of a typical rib.
- Rib 3-9
- Head – wedge shaped, 2 facet separated by crest of head – articulates with its own and superior vertebra
- Neck – Tubercle – articulate with transverse process and attachment of costotransverse lig
- Shaft/body- has costal groove.
- True Rib – Articulation with its own costal cartilage to sternum. True ribs are 1-7. False rib – articulate with sternum indirectly via their costal cartilage attaching to costal cartilage above in the costal margin. False ribs are 8-10. 11 and 12 is floating.
First rib
- Broadest and shortest and most curved of the true ribs
- Single facet on head for T1
- Anteriorly 2 groves on superior surface for SC artery(lat) and vein seperated by scalene tubercle.
Surface anatomy is important in the thorax.
- Manubrium – body of T3T4
- Sternal angle – T4T5 disc. 2nd costal cartilage
- Sternum -10cm long, lies ant to R heart border T5-9
- R side manubrium – overlies merging of brachioceph veins to form SVC – 1finger outside bone.
- SVC enters RA opp R 3rd costal cartilage
- Aortic arch. – L side of manubrium
- T4 nipple, T10 umbi.
- Trachea bifurcation – Transected by transverse thoracic plane when supine(T4/T5 disc)
- Oesophagus – Posterior structure – 25cm long
- Heart and its valves.
- Superior border – inferior border of left 2nd CC to r 3rd CC
- Right border – R 3cc to R 6th CC.
- Inferior boder – R 6 CC to L 5 CC at L MCL.
- Left border connects L 2nd CC to L 5 CC at MCL
- Valves are posterior to sternum
- Tricuspid – behind sternum at level of T4/5 intercostal space.
- Pulmonary – Left third costal cartilage
- Mitral – posterior to sternum at level of 4th costal cartilage
- Aortic – posterior to sternum at level of 3rd intercosral space.
- Pleura
- Visceral pleura covers lung parenchyma
- Parietal pleura – cervical cuppola 2-3cm above clavicle–> medially down mediastinum to hilum. R to CC 6 and L to CC4(then inferior to CC6), R8 in MCL and R10 in MAL, R12 at vertebra–> reflects on lung–> continues down to diaphragm and covers diaphragm –> ascend on costal wall and rejoins cervical cuppola.
- Horizontal fissure – from oblique fissure to Rib 4 and cc4.
- Oblique fissure – spinous process of T2 to 6CC anteriorly.
- Significant because there is the cardiac notch at CC4 for pericardiocentesis, costodiaphragmatic recesses(pleura go 2 rib spaces below in full expiration)
- Lung same start and medial as pleura but R6 at MCL, R8 at MAL, scapula line at R10 and finish following R10 to T10
Features of this Chest X-ray

http://lifeinthefastlane.com
Contents of intercostal space.
- V-A-N, or Intercostal vein-artery-nerve, from top to bottom
- several kinds of intercostal muscle
- intercostal lymph nodes
Intercostal space and layers in chest drain insertion
- 5th or 6th intercostal space in MAL
- Superiorly direct tube to remove air, inferiorly if for fluid.
- Skin subcutaneous tissue, external oblique, internal oblique aponeurosis, inner most oblique, parietal pleura.